WARNINGS AND PRECAUTIONS
Cytokine Release Syndrome (CRS)
Cytokine Release Syndrome (CRS) occurred following treatment with AUCATZYL. CRS was reported in 75% (75/100) of patients including Grade 3 CRS in 3% of patients. The median time to onset of CRS was 8 days following the first infusion (range: 1 to 23 days) with a median duration of 5 days (range: 1 to 21 days). The most common manifestations of CRS included fever (100%), hypotension (35%), and hypoxia (19%).
Prior to administering AUCATZYL, ensure that healthcare providers have immediate access to medications and resuscitative equipment to manage CRS. During and following treatment with AUCATZYL, closely monitor patients for signs and symptoms of CRS daily for at least 14 days at the healthcare facility following the first infusion. Continue to monitor patients for CRS for at least 4 weeks following each infusion with AUCATZYL. Counsel patients to seek immediate medical attention should signs or symptoms of CRS occur at any time. At the first sign of CRS, immediately evaluate the patient for hospitalization and institute treatment with supportive care based on severity and consider further management per current practice guidelines.
Neurologic Toxicities
Neurologic toxicities including Immune Effector Cell-associated Neurotoxicity Syndrome (ICANS), which were fatal or life-threatening, occurred following treatment with AUCATZYL. Neurologic toxicities were reported in 64% (64/100) of patients, including Grade ≥ 3 in 12% of patients. The median time to onset of neurologic toxicities was 10 days (range: 1 to 246 days) with a median duration of 13 days (range: 1 to 904 days). Among patients with neurologic toxicities, the most common symptoms (> 5%) included ICANS (38%), headache (34%), encephalopathy (33%), dizziness (22%), tremor (13%), anxiety (9%), insomnia (9%), and delirium (8%).
Immune Effector Cell-associated Neurotoxicity Syndrome (ICANS)
ICANS events occurred in 24% (24/100) of patients, including Grade ≥ 3 in 7% (7/100) of patients. Of the 24 patients who experienced ICANS, 33% (8/24) experienced an onset after the first infusion, but prior to the second infusion of AUCATZYL.
The median time to onset for ICANS events after the first infusion was 8 days (range: 1 to 10 days) and 6.5 days (range: 2 to 22 days) after the second infusion, with a median duration of 8.5 days (range: 1 to 53 days).
Eighty-eight percent (21/24) of patients received treatment for ICANS. All treated patients received high-dose corticosteroids and 42% (10/24) of patients received anti-epileptics prophylactically. Prior to administering AUCATZYL, ensure that healthcare providers have immediate access to medications and resuscitative equipment to manage ICANS.
Counsel patients to seek medical attention should signs or symptoms of neurologic toxicity/ ICANS occur. At the first sign of Neurologic Toxicity /ICANS, immediately evaluate patients for hospitalization and institute treatment with supportive care based on severity and consider further management per current practice guidelines.
Effect on Ability to Drive and Use Machines
Due to the potential for neurologic events, including altered mental status or seizures, patients receiving AUCATZYL are at risk for altered or decreased consciousness or coordination in the eight weeks following AUCATZYL infusion or until resolution of the neurological event by the treating physician. Advise patients to refrain from driving and engaging in hazardous occupations or activities, such as operating heavy or potentially dangerous machinery, during this initial period.
Prolonged Cytopenias
Patients may exhibit cytopenias including anemia, neutropenia, and thrombocytopenia for several weeks after treatment with lymphodepleting chemotherapy and AUCATZYL. In patients who were responders to AUCATZYL, Grade ≥ 3 cytopenias that persisted beyond Day 30 following AUCATZYL infusion were observed in 71% (29/41) of patients and included neutropenia (66%, 27/41) and thrombocytopenia (54%, 22/41). Grade 3 or higher cytopenias that persisted beyond Day 60 following AUCATZYL infusion was observed in 27% (11/41) of patients and included neutropenia (17%, 7/41) and thrombocytopenia (15%, 6/41). Monitor blood counts after AUCATZYL infusion.
Infections
Severe, including life-threatening and fatal infections occurred in patients after AUCATZYL infusion. Non-COVID-19 infections of all grades occurred in 67% (67/100) of patients. Grade 3 or higher non-COVID-19 infections occurred in 41% (41/100) of patients. AUCATZYL should not be administered to patients with clinically significant active systemic infections. Monitor patients for signs and symptoms of infection before and after AUCATZYL infusion and treat appropriately. Administer prophylactic antimicrobials according to local guidelines.
Grade 3 or higher febrile neutropenia was observed in 26% (26/100) of patients after AUCATZYL infusion and may be concurrent with CRS. In the event of febrile neutropenia, evaluate for infection and manage with broad-spectrum antibiotics, fluids, and other supportive care as medically indicated.
Viral reactivation, potentially severe or life-threatening, can occur in patients treated with drugs directed against B cells. There is no experience with manufacturing AUCATZYL for patients with a positive test for human immunodeficiency virus (HIV) or with active hepatitis B virus (HBV) or active hepatitis C virus (HCV). Perform screening for HBV, HCV and HIV in accordance with clinical guidelines before collection of cells for manufacturing.
Hypogammaglobulinemia
Hypogammaglobulinemia and B-cell aplasia can occur in patients after AUCATZYL infusion. Hypogammaglobulinemia was reported in 10% (10/100) of patients treated with AUCATZYL including Grade 3 events in 2 patients (2%).
Immunoglobulin levels should be monitored after treatment with AUCATZYL and managed per institutional guidelines including infection precautions, antibiotic or antiviral prophylaxis, and immunoglobulin replacement.
The safety of immunization with live viral vaccines during or following treatment with AUCATZYL has not been studied. Vaccination with live viral vaccines is not recommended for at least 6 weeks prior to the start of lymphodepleting chemotherapy treatment, during AUCATZYL treatment, and until immune recovery following treatment with AUCATZYL.
Hemophagocytic Lymphohistiocytosis/Macrophage Activation Syndrome (HLH/MAS)
HLH/MAS including fatal and life-threatening reactions occurred after treatment with AUCATZYL. HLH/MAS was reported in 2% (2/100) of patients and included Grade 3 and Grade 4 events with a time of onset at Day 22 and Day 41, respectively. One patient experienced a concurrent ICANS event after AUCATZYL infusion and died due to sepsis with ongoing HLH/MAS that had not resolved. Administer treatment for HLH/MAS according to institutional standards.
Hypersensitivity Reactions
Serious hypersensitivity reactions, including anaphylaxis, may occur due to dimethyl sulfoxide (DMSO), an excipient used in AUCATZYL. Observe patients for hypersensitivity reactions during and after AUCATZYL infusion.
Secondary Malignancies
Patients treated with AUCATZYL may develop secondary malignancies. T cell malignancies have occurred following treatment of hematologic malignancies with BCMA- and CD19-directed genetically modified autologous T cell immunotherapies. Mature T cell malignancies, including CAR-positive tumors, may present as soon as weeks following infusion, and may include fatal outcomes. Monitor lifelong for secondary malignancies. In the event that a secondary malignancy occurs, contact Autolus at 1-855-288-5227 for reporting and to obtain instructions on the collection of patient samples for testing.
Adverse Reactions
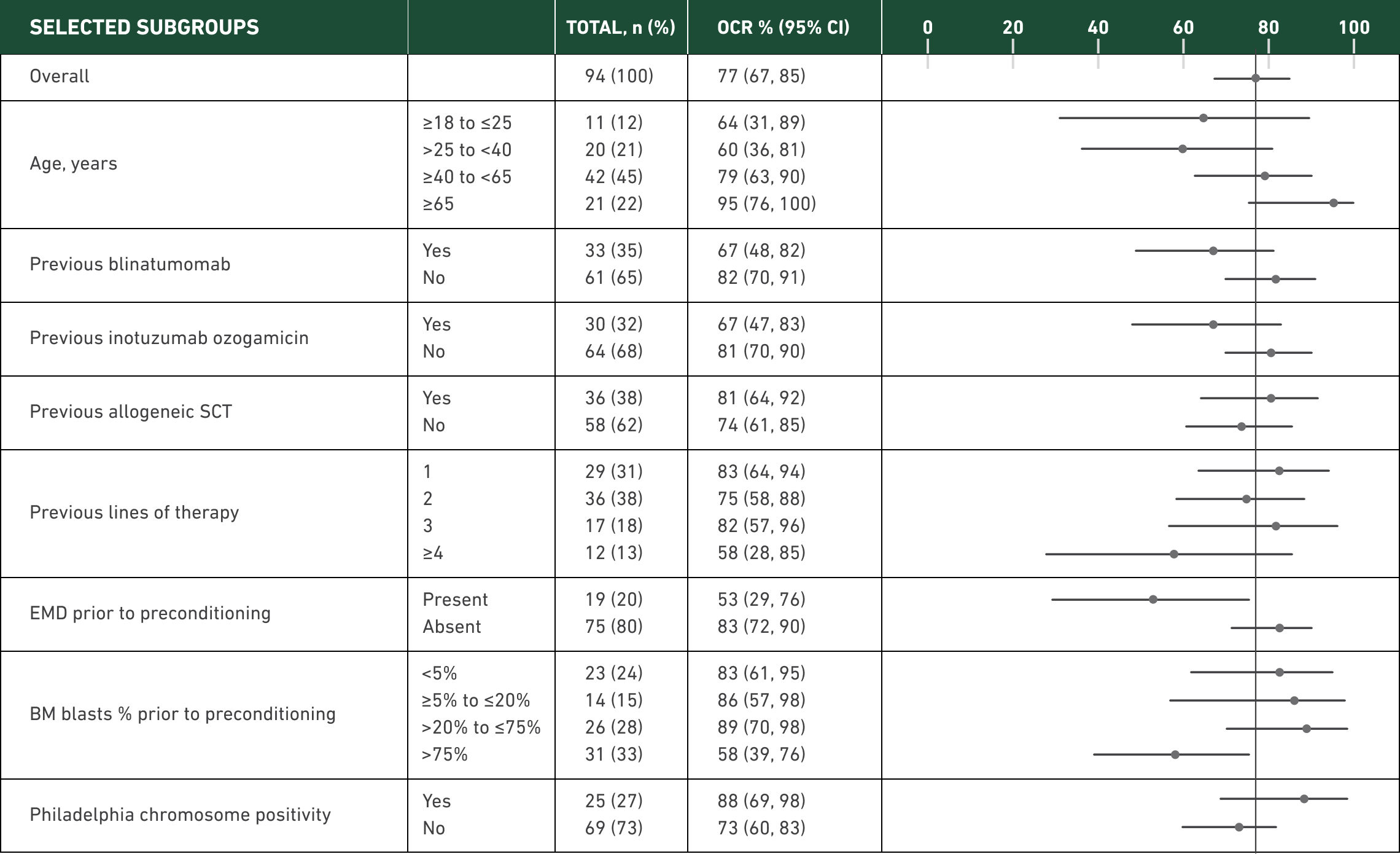
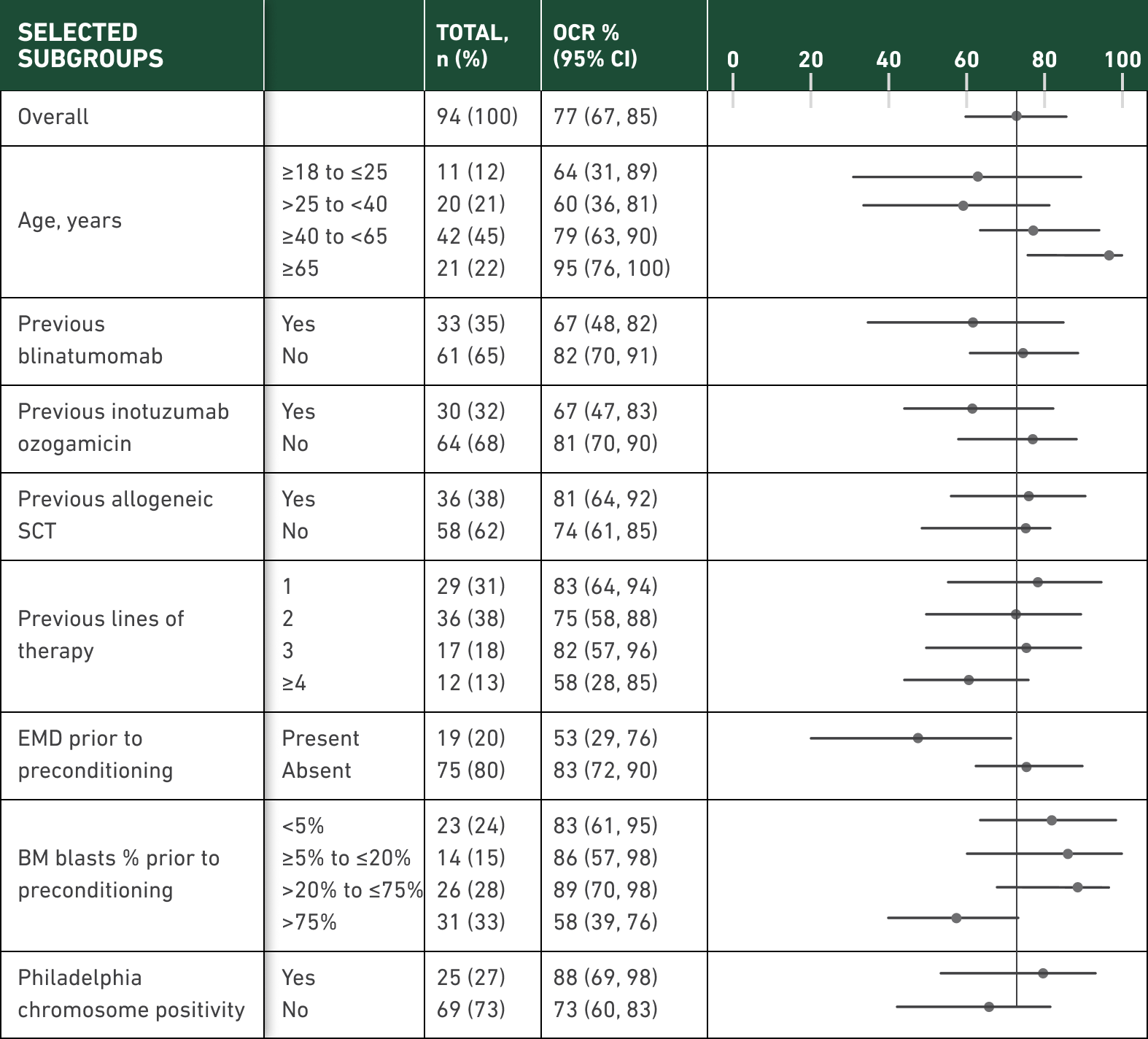
The safety of AUCATZYL was evaluated in the FELIX study in which 100 patients with relapsed or refractory B-cell acute lymphoblastic leukemia (B-ALL) received AUCATZYL at a median dose of 410 × 106 CD19 CAR-positive viable T cells (range: 10 to 480 × 106 CD19 CAR-positive viable T cells with 90% of patients receiving the recommended dose of 410 × 106 +/- 25%).
The most common serious adverse reactions of any Grade (incidence ≥ 2%) included infections-pathogen unspecified, febrile neutropenia, ICANS, CRS, fever, bacterial infectious disorders, encephalopathy, fungal infections, hemorrhage, respiratory failure, hypotension, ascites, HLH/MAS, thrombosis and hypoxia. Nine patients (9%) experienced fatal adverse reactions which included infections (sepsis, pneumonia, peritonitis), ascites, pulmonary embolism, acute respiratory distress syndrome, HLH/MAS and ICANS. Of the 9 patients, five patients who died from infections had pre-existing and ongoing neutropenia prior to receiving bridging therapy, lymphodepletion chemotherapy treatment and/or AUCATZYL.
Please see full Prescribing Information, including BOXED WARNING and Medication Guide.